
Introduction
Liver is a wedge shaped visceral organ in the body, occupies right hypochondrium, epigastric region and extends in to the left hypochondrium. It is divided by the presence of fossa for the gall bladder and groove for inferior vena cava in to right and left lobes, of which right lobe is larger than left lobe. It has quadrate and caudate lobes which are part of right lobe anatomically, but theoretically they are distinct.1
A thorough knowledge of anatomy of liver will avoid errors in diagnostic imaging and will also help the surgeons design appropriate surgical approaches.2 The variant morphology of liver can be either congenital or acquired. The congenital mal formations are atrophic or hypoplastic lobes, agenesis of lobes and fissures. The acquired malformations are as results of pressure exerted by the diaphragm or by nearby organ s and other peritoneal ligaments, which are related to liver.3
Accessory lobes have to be attended to when the vascular pedicles undergoes torsion or if metastasis occurs in them. Accessory lobes occur due to shift of the embryonic rudiment of the organ or it can be because there is septa which persists when it undergoes proliferation.4
The morphological variations of liver are of seven types as classified by Netter as shown in Table 1.5
A thorough knowledge of normal anatomy and its variations are highly significant during usage of imaging techniques and also during surgery.3 The objectives of this study is to determine the gross anatomical variations of the human liver in South Indian population.
Materials and Methods
This study was conducted in the Department of Anatomy of our Institution. A total of 35 numbers of liver removed from cadavers used for dissection for undergraduate students were used for the study. The removed livers were preserved in 10% formalin, the morphological variations of liver such as changes in size, shape, presence of accessory lobes, fissures, hypoplastic lobes were noted and tabulated. All the variations were photographed the results obtained were then tabulated.
Results and observations
The results are summarized are follows
Netter’s classification of morphological variations of liver.
Table 1 shows the 7 morphological classification of liver as classified by Netter.
Variations in fissures and lobes of the liver.
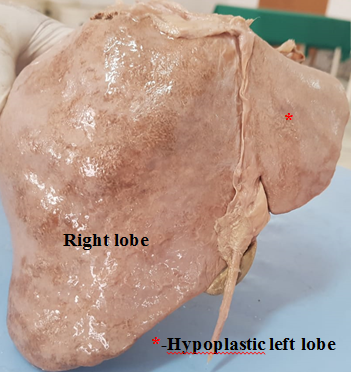
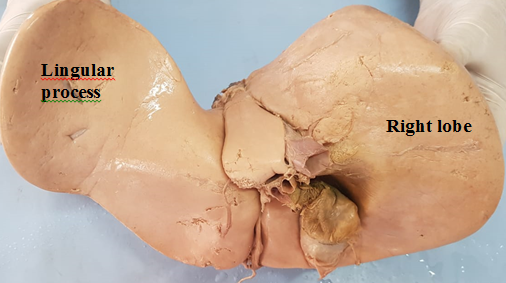
From Table 2 , it is observed t hat out of the 35 livers studied, 15 specimens (42.9%) exhibited normal fissures and lobes (Figure 1), 13 specimens (37.1%) had accessory fissures over different lobes (Figure 2). In 3 specimens (8.6%) of liver, hypoplastic left lobe was observed (Figure 3) and in 4 specimens (11.4%) lingular process of left lobe was observed (Figure 4).
Incidence of accessory fissures and accessory lobes – occurrence in various lobes of liver.
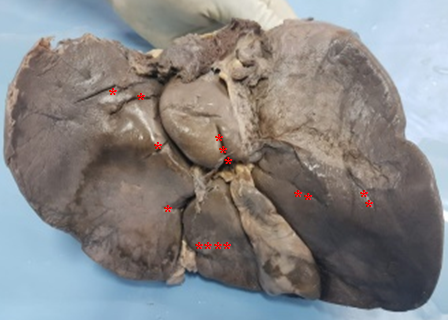
From Table 3, it is observed that 8 accessory fissures were seen in right lobe, 5 in left lobe, 4 in caudate lobe and 5 in quadrate lobe. One specimen of Liver showing accessory fissures over different lobes is shown in (Figure 2). Out of 35 livers studied, accessory lobes were observed in 9 liver specimens, which can be grouped as 1 in right lobe, 2 in left lobe, 5 in caudate lobe and 1 in quadrate lobe (Figure 5).
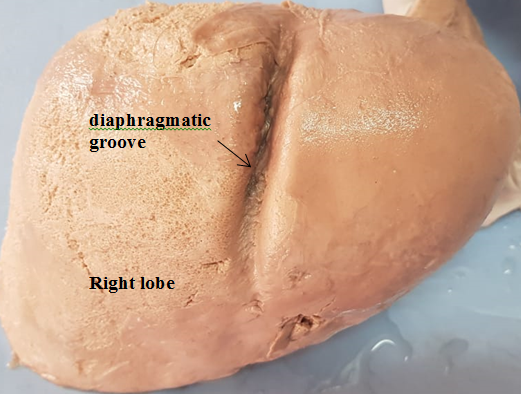
Occurrence of Diaphragmatic Groove:
In one specimen a deep diaphragmatic groove on superior surface of right lobe extending to the anterior surface (Figure 6) was observed.
Discussion
Congenital abnormalities of liver are very important as they guide us to uncover the underlying problems associated with the morphological anatomy of liver and as such these congenital malformations of liver are not very common. A thorough understanding of these in essential as these do not remain clinically silent. These have to be remembered preoperatively when making a diagnosis, as it will guide the Surgeons when he plans to operate on biliary tract or on Porto Caval anastomosis.6
Considering the development of Liver, Liver plates appear in the middle of 3rd week of development as a thickening of caudal part of forgut which grows to form hepatic bud which invaginates septum transversum7
As quoted by Wahane et al. liver in some lower animals (E.g. dogs and pigs) shows lobulated appearance separated by connective tissue and this can be applied to human liver by reversion. The human liver morphological variations can be classified as congenital or acquired, the congenital can be due to defect in development or due to excess growth during development. Excess growth during development leads to occurrence of accessory lobes of liver and this can pose wrong conclusions radiographically. In their study, wahane et al. studied 50 liver specimens and found accessory lobes and fissures in 16% and 20% respectively.8 In our study, the occurrence of accessory lobes were observed in 9 of the 35 specimens studied, i.e, in 25.7% of total specimen s. Accessory fissures were found in 13 of the 35 specimens i.e. in 37.1% of total specimens.
As quoted by Vinnakota et al. numerous accessory fissures of liver in ultrasound can be confused with macro nodular liver and hence a CT scan is further necessary for further correct diagnosis. In their study, they observed that 9 specimens had accessory fissure in quadrate lobe alone and in 1 specimen accessary fissure was present both in quadrate and caudate lobes and in another liver all the lobes right, left, caudate and quadrate lobes had accessary fissures on the undersurface.9 In our study accessory fissures were observed in 13 of the total number of specimens studied. These occurred in various lobes of Liver which can be grouped as 8 in right lobe, 5 in left lobe, 4 in caudate lobe and 5 in quadrate lobe.
Diaphragmatic sulci are formed because of pressure caused by groups of diaphragmatic muscles on the liver parenchyma which leads to irregular growth of liver and sulci formation. corrosion cast and radiological studies reveal that the sulci are nothing but portal fissures that represent poor zones of liver parenchyma adjacent to which are the portal territories. So the diaphragmatic sulci is indicative of the surface projection of portal fissure and also represent the hepatic veins with their tributaries passing through them.10 In our study, we observed in 2.9% of specimens the diaphragmatic sulci on the superior surface of right lobe extending to the anterior surface as compared to 7.5% observed by chaudhari et al.
As quoted by chin et al. for better patient outcomes, the correct knowledge of the morphological variations of liver are essential as there is increasing use of imaging techniques for diagnosis of diseases and laproscopy procedures. Though the variations of liver are silent, there are reported cases of clinical manifestations arising due to the variant morphology of liver.11
Table 1
Netter’s classification of morphological variations of liver.
Table 2
Variations in the fissures and lobes of the liver
Table 3
| Name of the lobe | Accessory fissures | Accessory lobes |
| Right lobe | 8 | 1 |
| Left lobe | 5 | 2 |
| Caudate lobe | 4 | 5 |
| Quadrate lobe | 5 | 1 |
Accessory fissures and Accessory lobes in various lobes of liver
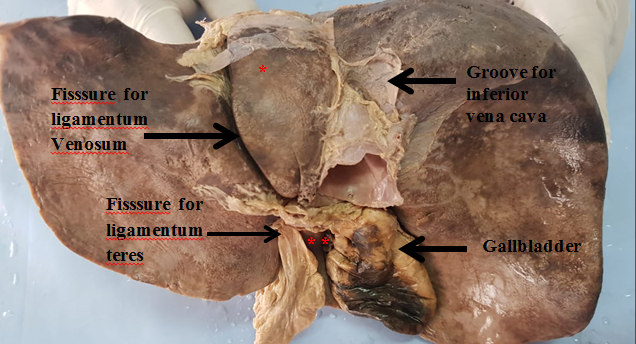
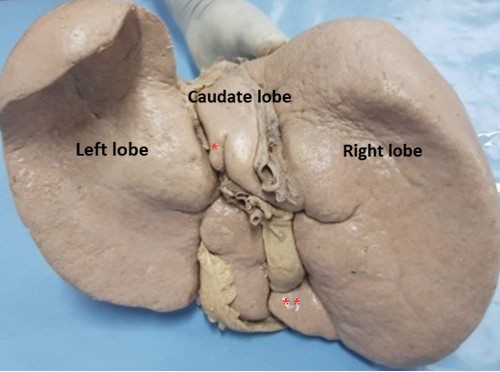
Figure 2
Accessory fissures in various lobes of Liver.
⃰ Accessory fissures over left lobe ⃰ ⃰ ⃰ Accessory fissures over right lobe ⃰ ⃰⃰ ⃰ Accessory fissures over caudate lobe
⃰ ⃰ ⃰ ⃰ Ac cessory fissures over quadrate lobe.
Conclusion
The authors conclude that morphological variations of liver must be taken in to account by the radiologist and gastroen terologist while making various differential diagnosis as these variations presents various clinical manifestation s/ implications, which can be observed because of their silent nature.