
Introduction
Among orthodontist Class II malocclusion still remain as a common and major challenge,1 it may be a skeletal or a dental component.2 Patient compliance is one of important success factors in orthodontic treatment.
Nevertheless, an orthodontist cannot always count on patient’s cooperation thus for more than three decades patient noncompliance has been a major concern in orthodontics, 3 and a number of publications since then affirm to continuing interest.
Fixed functional appliance treatment requires negligible patient compliance and can be grouped into various classifications based on their mode of action. Patients with Class II malocclusion can have a protrusion of maxilla or retrognathic mandible or combination of both along with aesthetic disorders and an abnormal dental relationship. Different orthodontic and orthopaedic approaches required for treating various malocclusions. In regular orthodontic practice functional appliance are widely used for treating Class II malocclusion cases.
McNamara 4 indicated that common feature of Class II malocclusion is a retrognathic mandible instead of prognathic maxilla. Advancement of mandible via functional appliance is frequently indicated in Class II malocclusion caused by retrusive mandible. 5, 6, 7, 8
Removable functional Appliances such as Twin block, Frankel, bionator, activator, can be used in patient in adolescent growth spurts9 and if patient appeared after the pubertal growth spurt or during the later stages of puberty various fixed functional appliances such as fixed twin block, Herbst appliance, jasper jumper, Universal bite jumper etc would be a better choice considering the patient compliance.
Development of various fixed functional appliances over decades led to the commencement of latest FFAs. Fixed functional appliance are “noncompliance Class II correctors”.10, 11 For noncompliance patients various fixed appliances have gained popularity in recent years among this one of such innovation is PowerScope,12 which is fundamentally a hybrid fixed functional appliance that is mainly used for correction of mild skeletal Class II cases in noncompliance patients.
PowerScope was developed by Dr. Andy Hayes who worked in concomitance with the American Orthodontics. Unalike other Class II correctors, there is no need for appliance manipulation or assembly measuring. 13, 14 as PowerScope also has the edge of permitting lateral movements due to its exclusive ball and socket joints and typical telescopic mechanism consisting of a Ni–Ti internal spring system which reduces the treatment time compared to the other Class II correctors. It also eradicates the need for special band assemblies or gingival headgear tubes and can be used with either bonded or banded tubes. It has a patient friendly design and a ready to use one-piece body in which no assembly or laboratory setup is required.
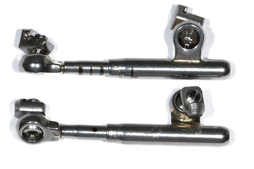
Properties of a PowerScope
Universal size for simple treatment application and easy inventory management (Figure 1).
It provides comfort fit for the patient because of its smooth and rounded edge design.
Patient acceptance as PowerScope features a low profile for an aesthetic.
It constitutes a nickel-titanium internal spring mechanism that provide 260 grams of force for continuous activation during treatment.
PowerScope’s telescopic system features three parts that will not detach during treatment thus helping to avoid unnecessary emergency visits.
Maximum lateral mandibular movement for improved patient comfort and acceptance because of its ball and socket joint.
Helps in reducing ulcer formation as no piston extends distally from the upper molars.
Components of a PowerScope
Locking nut attachment.
Telescopic system: An 18mm telescoping mechanism.
Hex-head screws: Situated at the upper and lower ends of the telescopic system.
NiTi spring: An internal spring that generates 260 g of force.
Crimpable shims: Available in sizes i.e. 1mm, 2mm or 3mm, mainly used for an initial activation and to reactivate the appliance during the treatment.
Hex-head driver.
Allen key type to tighten the screws.
PowerScope appliance installation
Appliance is placed distal to the canine of the mandibular arch and mesial to the first molar in the maxillary arch. Nuts attachment does not pinch the wire when installed. The system slides freely that can facilitate molars distalization in upper arch while in lower arch lower attachment nut has a “friction” fit as of the curvature found on the lower arch form with the transition from canine to premolar that mainly prevents the slamming of nuts in to canines.
Thus, PowerScope appliance provides simple installation and extensive range of motion, including patient comfort and acceptance which is a critical need of an orthodontist.
Case Report
A 14-years old male patient reported to clinic with chief complaint of forwardly placed upper front teeth.
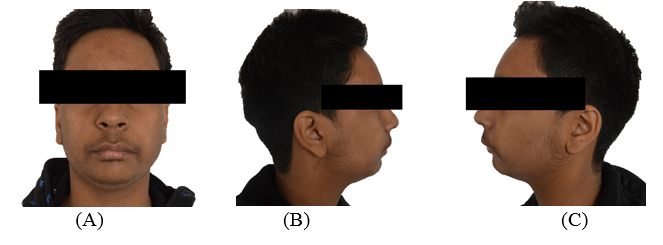
Extra oral examination showed protrusive upper lip along with a convex profile with posterior divergence and recessive chin, (Figure 2).
Intraoral examination revealed that the patient had a poor oral hygiene, All permanent teeth were present through second molar, A Class II canine relationship on the both right and left side was observed. A Class II Division 1 malocclusion with an overjet of 7 mm and an overbite of 6mm was observed. In relation with facial midline the lower midline was shifted 1 mm to the right. There was also 5.5-mm crowding in lower arch whereas 7mm of crowding was found to be in upper arch (Figure 3).

Lateral cephalogram and its tracing showed a convex skeletal profile. ANB angle of 6°, SNA-80°, SNB-74° along with a retrognathic mandible and a relatively normal positioned maxilla. An average growth pattern can be suggested from a normal mandibular plane angle of 25°. Dentoalveolar readings indicated a mild retroclined mandibular anteriors and proclination of upper anterior teeth (Figure 4).

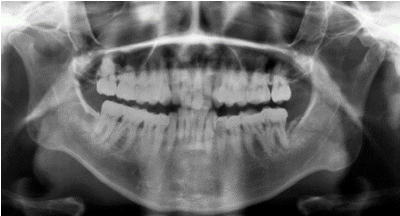
Panoramic radiograph revealed no bone pathology and a normal morphology of condyle. All permanent teeth are present through second molar with no major or severe decay of teeth (Figure 5).
Treatment objective
Non extraction approach to obtain an asymmetrical class I occlusion.
Advancement of mandible to improve overall facial aesthetics.
Alignment and levelling of teeth in both maxillary and mandibular arches and to obtain a functional occlusion.
Correcting the over jet.
Restricting the growth of maxilla in both vertical and sagittal plane.
Improvement of dental symmetry.
To achieve a balanced facial profile.
Treatment progress
Treatment began with using MBT appliance (0.022” slot). Levelling and alignment were carried out with 0.014” Niti wires followed by 0.017” X 0.025” and finally 0.019” x 0.025” Niti wires were used respectively. Total period for levelling and alignment was 7 months after which 0.019” × 0.025” stainless steel wire was placed in both the upper and lower arches followed by mandibular advancement using PowerScope appliance. Appliance was maintained until an unstrained Class I molar and Class I canine relation was obtained (Figure 6). Mandibular advancement led to significant and considerable improvement in facial profile of the patient. As PowerScope appliance was anchored on an orthodontic wire there was no requirement of debonding lower canine bracket or removing upper molar bands. Finally, treatment was completed with ideal arch wire sequencing followed by retention.

Discussion
For an orthodontist among various malocclusions, a Class II malocclusion presents a constant challenge. Various appliances and different orthodontic techniques including interarch appliances, extra-oral appliances, and surgical repositioning of the jaws have been introduced for correction of Class II malocclusion which can be as a result of skeletal abnormalities. Among interarch method Intermaxillary elastics are distinctively used for Class II correction, however for their effectiveness intermaxillary elastics anticipate heavily on patient compliance, and compliance in orthodontics is variable and highly difficult to predict. There could be an increase in treatment time and poor treatment results if patient cooperation is poor. Class II malocclusions due to mandibular retrusion are most commonly treated with functional orthodontic appliances. A functional appliance creates orthopaedic force directed at the mandibular condyle.
Functional appliances typically illustrate the tipping of the mandibular incisors, mesial movement of the mandibular molars, and variable effects associated with mandibular growth.
They can be of two types: removable or fixed appliances. 15, 16, 17, 18, 19 Among fixed functional appliance, PowerScope has been added to the inventory by American Orthodontics.
A PowerScope is a fixed one-piece appliance that is available in one size and suits all Class II cases. During jaw movements one-piece concept prevents removal of appliance. The appliance intercept bond failure of bracket and allows quick and easy wire-to-wire installation and it is customized with crimpable shims supplied along with the PowerScope armamentarium. Reduced patient discomfort and excellent jaw movement is observed due to ball and socket joint of the appliance. 20, 21 An unnecessary proclination of mandibular incisor is the most common dento alveolar demerit seen with PowerScope appliance though which can be avoided by a simple figure of ‘8’ consolidation of mandibular arch and lingual crown torque in anterior segment of the mandibular arch or simply through a cinch back of arch wire.
PowerScope appliance has specific edge over Class II elastics. This appliance provides push force distal to mandibular canine and mesial to maxillary molars through compressed niti spring. Activation of PowerScope mainly produce horizontal force that is slightly intrusive in nature whereas a Class II elastic deliver pull type of force and force is both horizontal and extrusive.22
Post cephalometric outcomes showed considerable enhancement in both dental and skeletal parameters were observed at the end of PowerScope treatment.
A noticeable mandibular advancement was seen as considerable reduction of 4° was observed in ANB angle from 6° to 2° post treatment, SNB angle increased from 74° to 78°, Beta angle improved from 26° to 29° and 4mm of improvement was seen in Wits appraisal also there was increase in mandibular length by 3mm, though no changes were observed in maxillary length after PowerScope appliance correction. Mild reduction in proclination of maxillary incisors was observed whereas mandibular incisors proclined by 4°angular and 2 mm linear (i.e. L1-NB : 29°,7mm) after correction via PowerScope (Figure 7).

Esthetic line in upper lip changes from 2 mm to 0 mm while a considerable -1mm to 2 mm in lower lip. No considerable change in Frankfurt mandibular plane angle from previous 25° to post 26° was observed suggesting normal direction of lower facial growth both horizontally and vertically. Effective improvement in nasolabial angle from 89° to 96° and Incisor mandibular plane angle from 94°to 99° post treatment (Figure 7) resulted in significant improvement in both skeletal and soft tissue profile of patient.
Forward repositioning in anterior direction of mandible was not itself caused by PowerScope appliance but it’s the internal spring that works when patient functions in a maximum intercuspation position. In present study a well‑balanced face with a pleasant smile which could be well ascertained from the superimposition of soft tissue and hard tissue was observed. The results were extremely satisfying as well as stable for both patient and clinician (Figure 8).

Conclusion
Clinical study leads to the following conclusion:
PowerScope correction leads to change in molar and canine to class 1 relationship.
There was no change in maxillary length though considerable advancement was seen in mandible.
Overjet and overbite reinstate to normal.
PowerScope leads to improvement of soft tissue profile.
Angulation of lower incisors are proclined to some extent.
Thus, PowerScope appliance could be effective in correcting Class II malocclusion specifically in non-compliance patients. Class II correction achieved along with a considerable improvement in both dental, skeletal as well as soft tissue parameters. PowerScope leads to forward positioning of the mandible leading to improvement in both aesthetic appearance and soft tissue profile of the patient.23
Table 1
Pre and post comparison of cephalometric findings