
Introduction
Introduction of Guglielmi detachable coil has changed the management of intractranial ruptured and unruptured aneurysm with lower initial morbidity and mortality rates. But coiling has been shown to have greater association with aneurysm recurrence, rebleeding and aneurysm remnant. However, the expansion of endovascular therapy has led to a significant increase in documented incidences of incomplete aneurysm obliteration, neck remnants, and recurrences, indicating an association between endovascular treatment and aneurysm rerupture in the current literature.1, 2, 3
Aneurysm recurrence after coil embolization remains both a major shortcoming of endovascular treatment and a daunting challenge for neurosurgeons without optimal management strategies. 4, 5, 6, 7 However, few data are available regarding the morphological changes of recurrent aneurysms and their management strategy.
We present a case of reruptured previously coiled anterior communicating artery aneurysm managed with microsurgical clipping.
Clinical History and Examination
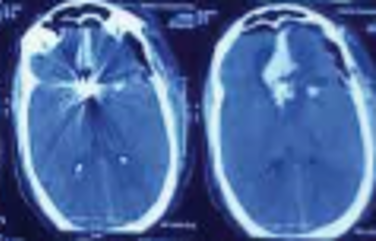
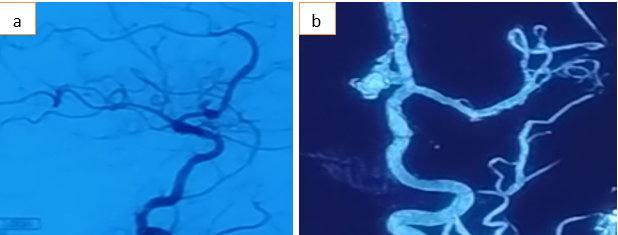
A 54-year-old male with history of coiling for Acom aneurysm 9 years back presented in the emergency with altered sensorium and right-sided haemiparesis. CTscan of the patient suggested a massive intra-cerebral bleed in the inter-hemispheric region (Figure 1). DSA showed ruptured ACOM Artery aneurysm and the coils were impacted at the neck of aneurysm and were seen extruding from the dome (Figure 2a, b). Challenges in planning the management - • It was a wide neck previously coiled ruptured aneurysm • Coils were seen impacted at the neck • Adjacent large haematoma
Patient was planned for surgical clipping of aneurysm. A left frontal-temporal craniotomy was performed. After gentle dissection of slyvian fissure and evacuation of frontal hematoma, the aneurysm appeared in full view.
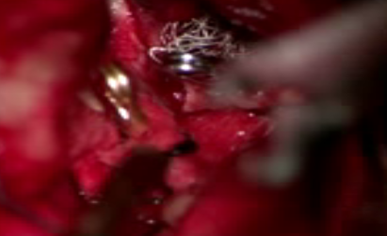
The dome of the aneurysm was adherent to surrounding brain parenchyma with thin translucent fragile wall (Figure 3). Coils were found encroaching over the neck lumen. After achieving proximal control, the dome was opened and the coils were gently pulled up, to relieve the impaction at the neck and then a permanent clip was applied at neck, securing the aneurysm (Figure 4). Coils were left inside the dome of aneurysm with wrapping of the dome with muscle (Figure 5). Patient did well in the post-operative period.


Discussion
Re-bleed after endovascular coiling occurs mostly within 1 year, with 50% cases reported between 1-3 days. These cases generally carry a high mortality and morbidity rates. Recoiling of recurrent aneurysm comes with its own risk of extrusion of coils, coil compaction, rupture and regrowth of aneurysm. Microsurgical clipping stands as an alternate to recurrent previously coiled aneurysm, but certain conditions make clipping a challenge such as coil mass making it difficult to achieve full occlusion of neck, coil extrusion and availability of minimal neck. The treatment in this case was challenging and no clear guidelines are available as very few cases are reported in the literature. This patient was managed surgically with clipping after a lot of meticulous planning.
Conclusion
Microsurgical clipping is an effective intervention for managing reruptured previously coiled intracranial aneurysm.